Premenstrual Syndrome (PMS)
Menstruating women often experience serious hormonal changes throughout the month. Customizing their nutrition program to account for these changes can be of great benefit for these women. One of our consultants has done this for 16 years with excellent results in slow oxidizers. Here is the basic plan, followed by its explanation.
It is important to take into account that this newsletter addresses serious cases of PMS and therefore requires variations in the normally suggested supplement programs.
Customizing The Program
We used to call this the PMS program, but it is more than that. It involves three phases of the monthly cycle and appropriate program changes for each phase. It is easy to teach your female patients about these changes, or just copy this newsletter for them.
- When the period begins (3 to 5 days), hormone levels are lowest. Menstruating women may benefit from more stimulating, sodium-raising supplements such as B vitamins, manganese, glandulars, higher-doses vitamin B6 and digestive enzymes. Do not take zinc, magnesium, taurine, inositol, choline and molybdenum at this time. Too much zinc or molybdenum, for example, may extend the bleeding by lowering copper and estrogen.
- After the bleeding stops, go on the regular recommended nutrition program.
- Premenstrually (7-10 days before the period), most women will feel much better taking supplements that lower the sodium/potassium ratio. A good program is: B6, magnesium, zinc and digestive enzymes. At this time, avoid taking B-complex vitamins and glandulars which are more stimulating.
In summary, when the hormones are low, the sodium-raising nutrients (vitamin C and E, B complex, manganese and glandulars) are excellent. Premenstrually, the sodium-lowering nutrients (zinc and magnesium) are better. Vitamin B6 is good for both. Molybdenum may not be best either premenstrually or during the menstrual flow, although it may be excellent the rest of the month.
Basic Physiology
The chart of the hormonal changes is helpful to keep in mind. Some women are aware of the monthly changes, while others are not. This is often due to poor health or other fluctuations such as blood sugar changes that overshadow the monthly changes.
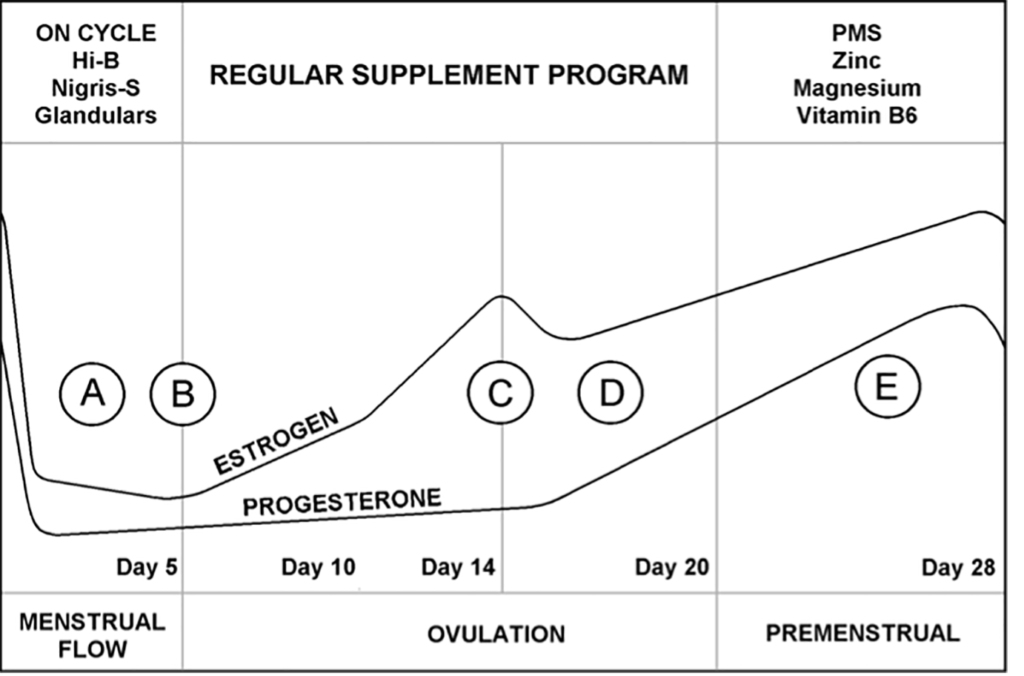
Refer to the chart of monthly hormonal changes. During menstrual bleeding, (A), estrogen, progesterone and copper levels are very low. The drop in the levels actually causes bleeding to begin and continue. At the end of the bleeding phase, (B), estrogen begins to rise. Estrogen continues to rise until ovulation, (C) about half way through the cycle. It takes a short dip and then continues to rise during the second half of the cycle, (D). Progesterone begins to rise as well in the second half of the cycle. Copper levels tend to parallel estrogen levels and rise as the cycle progresses.
In the premenstrual phase (E), 7-10 days before the period, copper and estrogen are high giving rise to PMS symptoms in many women. When the period begins, estrogen, progesterone and copper levels fall rapidly to begin the cycle once again. (See chart below)
Stress and the Menstrual Cycle
The rise and fall of the female hormones and copper level during the month places added stress on a woman's body. Healthy women who have adequate adaptive energy may tolerate the changes without too much discomfort. Those with weak adrenal glands, copper and mercury toxicity, or other biochemical imbalances often find the added work creates severe symptoms.
The liver may be unable to metabolize the extra hormones, the body cannot eliminate the excess minerals, and the added stress aggravates other imbalances. The goal of customizing the program for the menstrual cycle is to reduce biochemical stress.
High and Low Estrogen PMS
There is another theory of PMS that deserves mention, though our consultants have found it less useful. Dr. Katherine Dalton, MD and others have identified high estrogen and low estrogen PMS. The two types can alternate if one ovary produces more hormones than the other.
We associate the high estrogen type with a high hair sodium/potassium ratio, high copper and symptoms of water retention, anger, irritability and breast tenderness. The low estrogen type is more associated with a low sodium/potassium ratio, biounavailable copper and symptoms of depression and exhaustion.
In practice, tailoring the program to the three stages of the monthly hormonal changes as described above has been found more useful than the high and low estrogen theory of PMS.
Correcting Underlying Imbalances
In addition to customizing the program for the time of the month, correcting underlying imbalances that contribute to PMS is very important. A primary area is the diet, which is often too rich in carbohydrates and low in protein. Correcting the diet is very helpful for menstruating women.
Fatigue, due to a stressful lifestyle, emotional imbalances, lack of adequate support, exercise or rest and other stress factors definitely affects the menstrual cycle. This in turn affects the liver's ability to metabolize estrogen and affects the adrenal glands which produce female hormones, and which regulate copper metabolism and energy production.
Correction of PMS is best when it involves a total approach with dietary correction, customized supplements and lifestyle improvements.
The preceding statements have not been evaluated by the
Food and Drug Administration
This information is not intended to diagnose, treat, cure or prevent any disease.